Slow-release lithium was perhaps a myth / Priadel to be discontinued in the UK
September 7, 2020 Leave a comment

I am slightly saddened that the Priadel brand of lithium carbonate is to be discontinued in the UK, as that was the only brand I took every evening from 1998 to 2011 (other than a year taking 200mg Priadel with 450mg Camcolit).
Some lithium carbonate tablets have been described as ‘slow-release’ or ‘sustained release’ but what does this mean?
When researching for our handbook for nurses, we found that blood taken from patients at hourly intervals showed a rise in blood lithium in the first few hours after taking the lithium carbonate and then the level falling again. It worked out that when lithium is taken at bedtime the maximum in the person’s blood is likely to occur early in the morning and can already be dropping at the time when a blood sample would normally be taken at the doctor’s surgery the next morning.
This means that the timing of blood tests will, to some extent, influence the result. It also means that a ‘safe’ high reading in blood taken mid-morning is no guarantee that levels were not ‘toxic’ a few hours earlier.
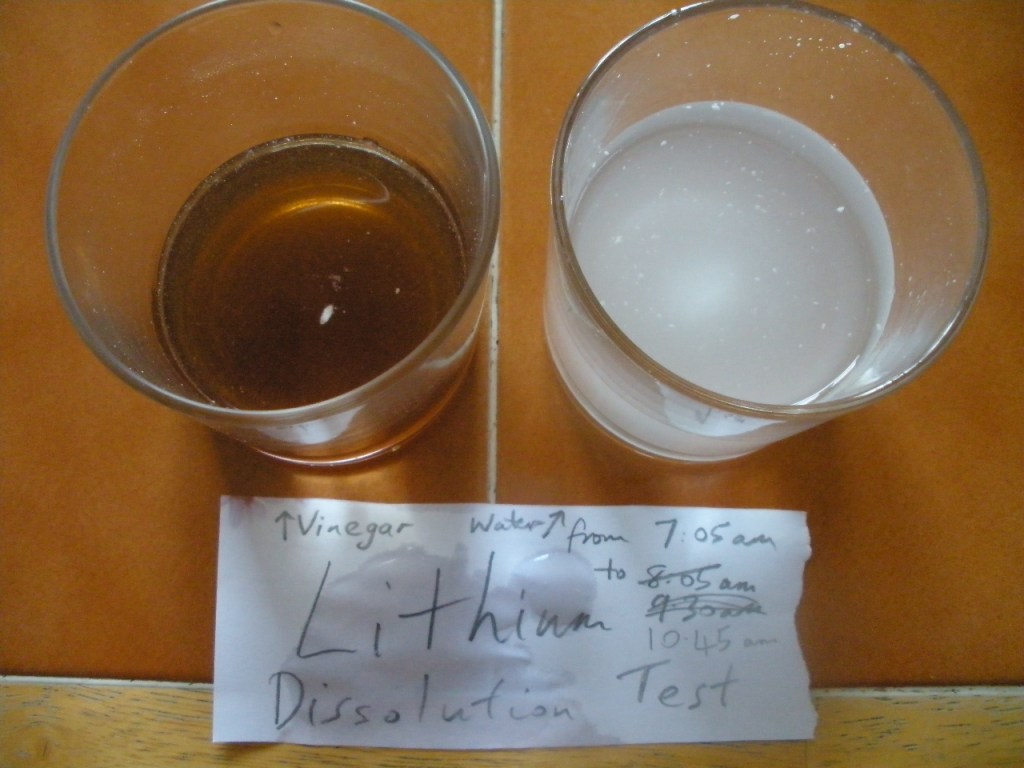
Carbonates tend to dissolve quicker in acid (such as stomach acid) than in water. To get an idea of how much quicker I dropped a 400mg Priadel tablet into a glass of water and a glass containing vinegar. As the photograph above shows the tablet dispersed quickly in water and even quicker in the acidic vinegar.
Are any lithium carbonate tablets really slow-release? I think not, and that I think is why no significance difference was found between Priadel ‘slow-release’ and Camcolit (that at the time of testing was not claiming to be slow-release).
Whether or not all or no lithium carbonate tablets are described as slow release, those who need or choose to continue to use lithium carbonate are likely to be fine when they need to change, from Priadel, to one of the other brands sometime before April 2021.
Here is part of a discussion of this from: The Pharmaceutical Journal “the overall outcome was that Priadel 400mg tablets were “sustained release” but had the same release as Camcolit 400mg plain tablets (the comparator in the Priadel study), Camcolit 400mg was then labelled sustained-release too. It wasn’t, but if the release was identical to the so-called ‘sustained release tablet’,” Stephen Bazire22 AUG 2020